 This picture is by Darryl Leja, NHGRI. It is in the public domain at http://www.genome.gov
This picture is by Darryl Leja, NHGRI. It is in the public domain at http://www.genome.gov
Should you and your family be tested for genetic conditions that can cause blood clots? After you have had a pulmonary embolism or DVT (deep vein thrombosis) you may think that the answer is an easy, “YES!” It isn’t. Genetic testing comes at a price. You need to know what that price is and if you are willing to pay it. You also need to know if you are willing to make that decision for your children and other family members. Get ready for a quick ride through genetics, genetic testing, and the dark side of testing for genetic blood clotting conditions.
Blood clotting conditions raise the risk of forming blood clots in the lungs (pulmonary embolism) or in the large veins in your body (deep vein thrombosis). These clots can be very serious and often have a lengthy recovery period. Sometimes these clots are fatal.
We can break clotting conditions into two general groups: genetic and non-genetic. Genetic clotting conditions come from one of your parents by way of the genes that were carried in an egg or sperm cell when you were conceived. Non-genetic clotting conditions do not come from your parents. These can come from things like cancer, other diseases, or things that we haven’t discovered yet. We are going to focus on the first group, clotting conditions that are caused by genetics.
When you were conceived you received genetic material from your mother and father. For instance, I have blue eyes. I have one gene for blue eyes from my mother and one gene for blue eyes from my father. I also have a clotting condition called Factor V Leiden. I have one good copy of the Factor V Leiden gene. It came from my mother. I also have one mutated gene from my father. (We will come back to this a little later.)
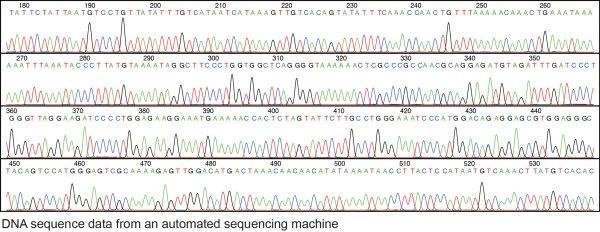
Your DNA looks a bit like a spring shaped ladder. It is made up of 4 chemicals that we typically refer to in an abbreviated form: A, G, T, and C. Each ladder rung has a pair of letter with one side from mom and the other side from dad. Each ladder rung is responsible for an instruction about who and what you are. Scientists have mapped out these ladder rungs. Each step is a location and each location has certain patterns of A, G, T, C that are acceptable. If just one of those letters is off, your genetic code has a “mutation”. Mutations may do something small like change your hair color. Unfortunately, mutations can also do something more serious like impacting how your blood clots. These blood clotting mutations are what doctors are looking for when they run tests for genetic blood clotting conditions.
Genetic testing takes some material from your body, pulls out the DNA, and then looks at certain sections of that DNA to see if it has the correct chemicals in the correct places. For example, one wrong letter in this section of DNA causes Factor V Leiden: GCAAGAACTGCAGGGGAGGAGGACGCTGCCACCCACAGCCTCTAGAGCTCATTGCAGCTGGGACAGCCCGGAGTGTGGTTATGTTTGGGCTATTATCTAATGCTGTGTAGAAATATTAAAACCCCTGTTATTTTGAAATAAAAAAGATACCCACTTTT. A DNA test scans for mistakes and uses them to identify any clotting conditions.
DNA testing has a number of benefits. First, these tests are very accurate because your DNA never changes. You get your DNA at conception and you have the same DNA throughout every cell in your body your entire life. Blood clots and anticoagulation will not change your DNA. Second, DNA tests may also help other family members understand any increased blood clots risks. As DNA is passed through parents to offspring you can figure out who should watch carefully for clots without having them tested. Lastly, DNA testing can be done before something goes wrong. Your doctor can test you and warn you of potential health issues before they happen. This gives you a chance to avoid problems that faulty DNA may cause.
So, if DNA testing is so useful, why am I writing an article about the dark side of genetic testing? Knowing your DNA comes at a cost. You may learn that you or your family member has an incurable condition. You may pay for a test that doesn’t matter because the disease never would have showed up in that person. (Factor V Leiden only has a 1 in 10 chance of causing a clot!). DNA testing may cause unneeded fear and stress. Low risk clotting conditions typically are not medicated as the medication is higher risk than the chance of serious illness from a clot. Someone may end up taking unneeded medication and have serious side effects. Medical treatment after genetic testing isn’t always clear.
Health isn’t the only risk with DNA testing. There is another very large and very real risk with genetic testing, discrimination. In 2008 the Genetic Discrimination Nondiscrimination Act (GINA) was enacted to protect Americans from job and medical insurance discrimination from results of genetic testing. GINA ensures that health insurance companies cannot ask you about any DNA testing or any DNA test results when you apply for insurance. GINA also states that employers may not ask for the results of DNA testing when making hiring or promotion decisions. GINA is a good start but there are still many places that can discriminate based on genetic test results.
Genetic discrimination can still be found in many places. Life insurance, annuities, banks, home insurance, travel insurance, and disability insurance can all review the results of past DNA testing before determining eligibility. It doesn’t matter when the testing occurred. A parent may have a 6-year-old child tested for genetic clotting conditions. When the child is 46 that genetic information may still disqualify him or her from participating in certain services. Your DNA never changes so the results of a DNA test will follow you forever, even if you were not the person that decided to have the test done. Another place discrimination shows up is in subconscious discrimination. A possible date might turn a woman down to blood clot risks in pregnancy. You may be passed over for a job after your workplace hears about your results because your boss is subconsciously concerned that stress may cause clots. Some of these forms of discrimination are obvious, some are not. They all share one thing in common: they are a result of a DNA test.
DNA testing is often used when blood clots occur. DNA testing can help you to determine your treatment. It can also help family members avoid future clots. The problem is that genetic testing, like all medical procedures, should be weighed carefully. Some people want to have all of their children and close family members tested. I recommend talking to different doctors before jumping into family blood testing. If the blood testing will have a significant impact in medical treatment it may be warranted. On the other hand, if the DNA test is being used as nothing more than a precaution, you may decide that your own clotting history is enough precaution on its own. Ask your doctor how treatment will change based on the DNA test results. The social and monetary costs must be determined and considered.
Back to my story...
After my clots in 2008 we decided not to have my parents tested. As a family we did inform other family members of my medical history and Factor V Leiden diagnosis so that they could be on the lookout for clots and could enact clot prevention strategies. Since then both of my parents had surgery. While the doctor didn’t require it, they chose to have Factor V Leiden testing. My dad was my gene donor. It didn’t change their surgeries much. My mom who does not have Factor V Leiden was given pressure cuffs and anticoagulation as she had a high risk surgery. My dad’s surgery was much less serious and had the pressure cuffs while in surgery. Thankfully, neither clotted.
For more information about genetic testing I highly recommend an episode of Neil DeGrasse Tyson’s podcast called Star Talk. Season 7, episode 9 is titled The Promise and Peril of the Genomic Revolution. It features one of the founders of 23 and Me and discusses the morality and future of genetic testing. This episode can be found here: https://soundcloud.com/startalk/the-promise-and-peril-of-the-genomic-revolution or you can listen to it below.
Blood clotting conditions raise the risk of forming blood clots in the lungs (pulmonary embolism) or in the large veins in your body (deep vein thrombosis). These clots can be very serious and often have a lengthy recovery period. Sometimes these clots are fatal.
We can break clotting conditions into two general groups: genetic and non-genetic. Genetic clotting conditions come from one of your parents by way of the genes that were carried in an egg or sperm cell when you were conceived. Non-genetic clotting conditions do not come from your parents. These can come from things like cancer, other diseases, or things that we haven’t discovered yet. We are going to focus on the first group, clotting conditions that are caused by genetics.
When you were conceived you received genetic material from your mother and father. For instance, I have blue eyes. I have one gene for blue eyes from my mother and one gene for blue eyes from my father. I also have a clotting condition called Factor V Leiden. I have one good copy of the Factor V Leiden gene. It came from my mother. I also have one mutated gene from my father. (We will come back to this a little later.)
Your DNA looks a bit like a spring shaped ladder. It is made up of 4 chemicals that we typically refer to in an abbreviated form: A, G, T, and C. Each ladder rung has a pair of letter with one side from mom and the other side from dad. Each ladder rung is responsible for an instruction about who and what you are. Scientists have mapped out these ladder rungs. Each step is a location and each location has certain patterns of A, G, T, C that are acceptable. If just one of those letters is off, your genetic code has a “mutation”. Mutations may do something small like change your hair color. Unfortunately, mutations can also do something more serious like impacting how your blood clots. These blood clotting mutations are what doctors are looking for when they run tests for genetic blood clotting conditions.
Genetic testing takes some material from your body, pulls out the DNA, and then looks at certain sections of that DNA to see if it has the correct chemicals in the correct places. For example, one wrong letter in this section of DNA causes Factor V Leiden: GCAAGAACTGCAGGGGAGGAGGACGCTGCCACCCACAGCCTCTAGAGCTCATTGCAGCTGGGACAGCCCGGAGTGTGGTTATGTTTGGGCTATTATCTAATGCTGTGTAGAAATATTAAAACCCCTGTTATTTTGAAATAAAAAAGATACCCACTTTT. A DNA test scans for mistakes and uses them to identify any clotting conditions.
DNA testing has a number of benefits. First, these tests are very accurate because your DNA never changes. You get your DNA at conception and you have the same DNA throughout every cell in your body your entire life. Blood clots and anticoagulation will not change your DNA. Second, DNA tests may also help other family members understand any increased blood clots risks. As DNA is passed through parents to offspring you can figure out who should watch carefully for clots without having them tested. Lastly, DNA testing can be done before something goes wrong. Your doctor can test you and warn you of potential health issues before they happen. This gives you a chance to avoid problems that faulty DNA may cause.
So, if DNA testing is so useful, why am I writing an article about the dark side of genetic testing? Knowing your DNA comes at a cost. You may learn that you or your family member has an incurable condition. You may pay for a test that doesn’t matter because the disease never would have showed up in that person. (Factor V Leiden only has a 1 in 10 chance of causing a clot!). DNA testing may cause unneeded fear and stress. Low risk clotting conditions typically are not medicated as the medication is higher risk than the chance of serious illness from a clot. Someone may end up taking unneeded medication and have serious side effects. Medical treatment after genetic testing isn’t always clear.
Health isn’t the only risk with DNA testing. There is another very large and very real risk with genetic testing, discrimination. In 2008 the Genetic Discrimination Nondiscrimination Act (GINA) was enacted to protect Americans from job and medical insurance discrimination from results of genetic testing. GINA ensures that health insurance companies cannot ask you about any DNA testing or any DNA test results when you apply for insurance. GINA also states that employers may not ask for the results of DNA testing when making hiring or promotion decisions. GINA is a good start but there are still many places that can discriminate based on genetic test results.
Genetic discrimination can still be found in many places. Life insurance, annuities, banks, home insurance, travel insurance, and disability insurance can all review the results of past DNA testing before determining eligibility. It doesn’t matter when the testing occurred. A parent may have a 6-year-old child tested for genetic clotting conditions. When the child is 46 that genetic information may still disqualify him or her from participating in certain services. Your DNA never changes so the results of a DNA test will follow you forever, even if you were not the person that decided to have the test done. Another place discrimination shows up is in subconscious discrimination. A possible date might turn a woman down to blood clot risks in pregnancy. You may be passed over for a job after your workplace hears about your results because your boss is subconsciously concerned that stress may cause clots. Some of these forms of discrimination are obvious, some are not. They all share one thing in common: they are a result of a DNA test.
DNA testing is often used when blood clots occur. DNA testing can help you to determine your treatment. It can also help family members avoid future clots. The problem is that genetic testing, like all medical procedures, should be weighed carefully. Some people want to have all of their children and close family members tested. I recommend talking to different doctors before jumping into family blood testing. If the blood testing will have a significant impact in medical treatment it may be warranted. On the other hand, if the DNA test is being used as nothing more than a precaution, you may decide that your own clotting history is enough precaution on its own. Ask your doctor how treatment will change based on the DNA test results. The social and monetary costs must be determined and considered.
Back to my story...
After my clots in 2008 we decided not to have my parents tested. As a family we did inform other family members of my medical history and Factor V Leiden diagnosis so that they could be on the lookout for clots and could enact clot prevention strategies. Since then both of my parents had surgery. While the doctor didn’t require it, they chose to have Factor V Leiden testing. My dad was my gene donor. It didn’t change their surgeries much. My mom who does not have Factor V Leiden was given pressure cuffs and anticoagulation as she had a high risk surgery. My dad’s surgery was much less serious and had the pressure cuffs while in surgery. Thankfully, neither clotted.
For more information about genetic testing I highly recommend an episode of Neil DeGrasse Tyson’s podcast called Star Talk. Season 7, episode 9 is titled The Promise and Peril of the Genomic Revolution. It features one of the founders of 23 and Me and discusses the morality and future of genetic testing. This episode can be found here: https://soundcloud.com/startalk/the-promise-and-peril-of-the-genomic-revolution or you can listen to it below.


 RSS Feed
RSS Feed

